Diabetes after SARS-CoV-2 Vaccination
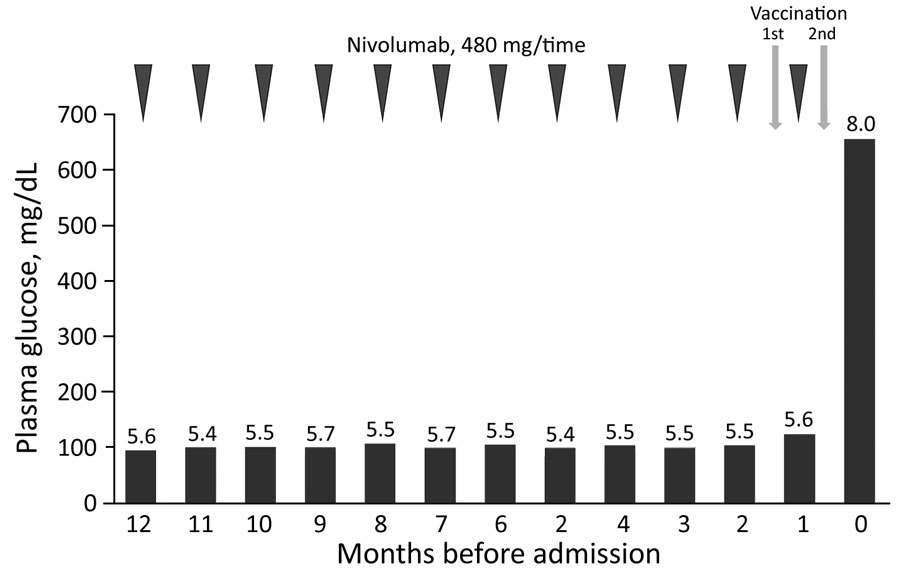
A 43-year-old man who had malignant melanoma (pT3bN1bM0 stage IIIC) received nivolumab treatment (480 mg 1× every 4 wks) 12 months before admission. Fasting plasma glucose level was 94 mg/dL and glycated hemoglobin (HbA1c) 5.6% at treatment initiation. Plasma glucose and HbA1c were tested every 4 weeks. His range of plasma glucose was 90–123 mg/dL and that of HbA1c was 5.4%–5.7% (Figure). Positron emission tomography–computed tomography showed no metastasis or recurrence of the tumor 1 month before admission.
The man received his first SARS-CoV-2 vaccination 35 days before admission. No apparent adverse reactions occurred, except for local pain. The last nivolumab dose was administered 21 days before admission and the second SARS-CoV-2 vaccination 14 days before admission. The next day, he had a slight fever (temperature 37°C), which soon subsided. Thirst, polydipsia, and polyuria appeared 2 days after the second vaccination. He started drinking 3 L of water/day, and his weight decreased by 5 kg over the next 12 days.
Twelve days after the second vaccination, his blood glucose level was 655 mg/dL and his HbA1c 8.0%. Levels of ketone bodies increased; 3-hydroxybutyric acid was 2,813 μmol/L and acetoacetate 1,936 μmol/L. He was urgently admitted to the hospital because of a diagnosis of ICI-associated T1D and marked ketosis.
REFERENCE
Sato T, Kodama S, Kaneko K, Imai J, Katagiri H. Type 1 diabetes mellitus associated with nivolumab after second SARS-CoV-2 vaccination, Japan. Emerg Infect Dis. 2022 Jul [date cited]. https://doi.org/10.3201/eid2807.220127
Original Publication Date: April 25, 2022



Comments
Post a Comment